There are some really valid and thought provoking points made by several contributors to this thread and I look forward to reading more in the coming days. However, what I hope most of all is that we continue to be respectful to each other. Play the ball not the man.
6 Likes
Good post @neilw.
Just to address this one point:
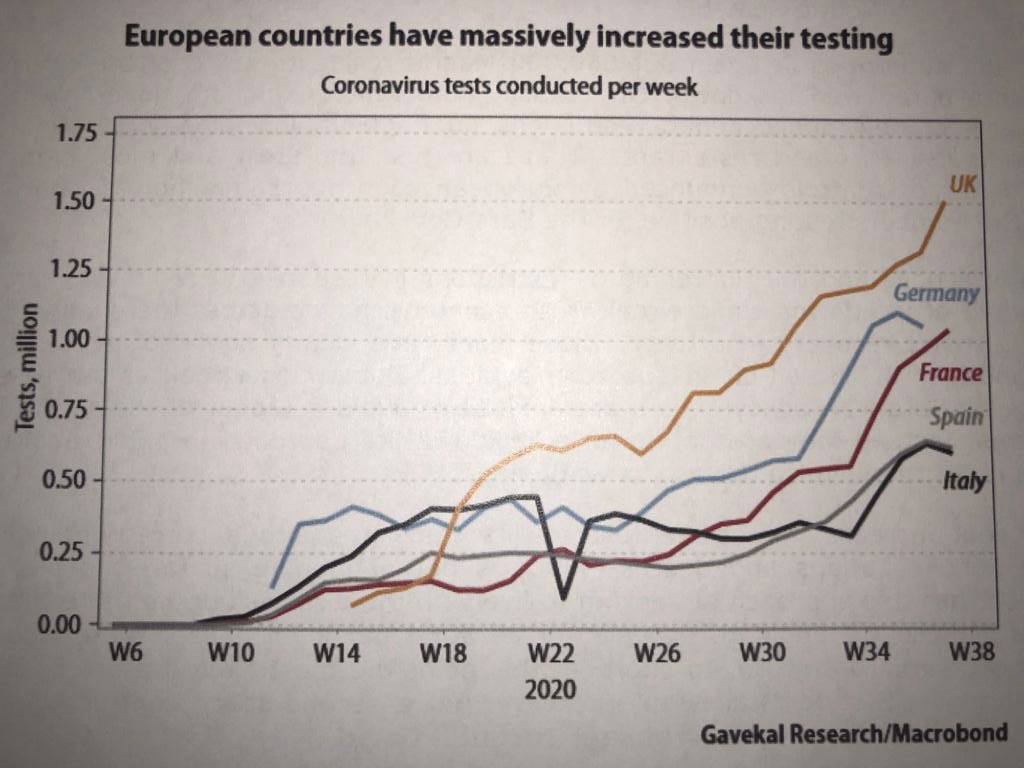
We hear a lot from the mainstream media about the UK’s supposed failings, and rarely our successes. But our testing has been streets ahead of the rest of Europe for a while now:

3 Likes
And we can all agree to disagree. There are no winners in this covid nightmare
3 Likes
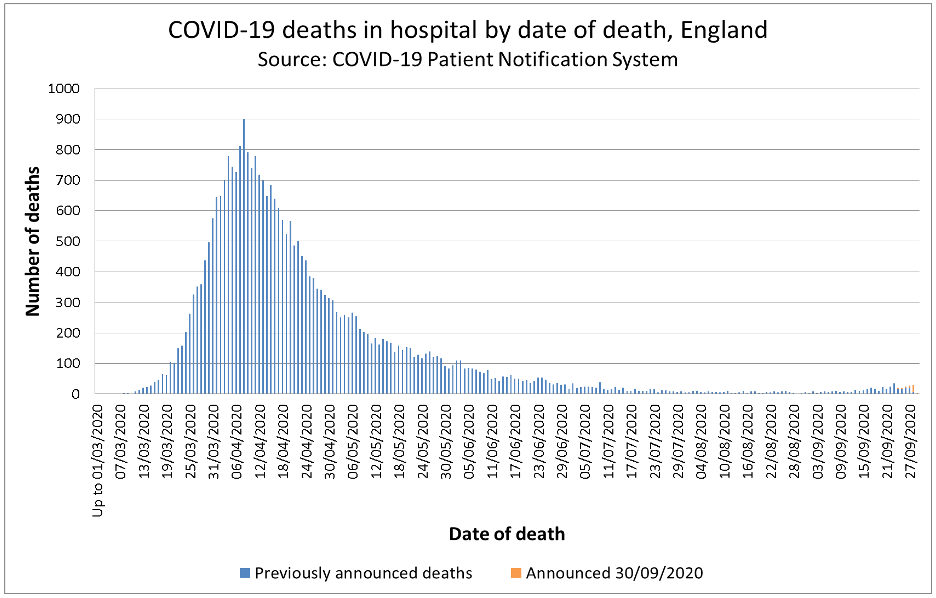
As at 16 September, the number of Covid-related deaths in England involving individuals under 60 and who had no existing medical condition was 309. And, for many of these, Covid may not have been the thing that actually killed them.
This is from https://www.england.nhs.uk/statistics/statistical-work-areas/covid-19-daily-deaths/
and before all the virtue signallers get foamed up, this shows the insanity of what is going on. At a colossal and often unrecoupable cost we have protected everyone when we could have prioritised the few most at risk.
Thank you for sharing the info, learning lots!
A question on the over 60s- do you know the % who already have underlying conditions vs not? I imagine it’s not so easy to get that info, but reason I ask is because I don’t consider 60 to be old in the slightest. So I wonder whether those falling in that age group with no underlying conditions would generally fare in a less strict set of rules - many of which are full time working, commuting, etc…
1 Like
Does anyone know how ‘existing condition’ is defined as in the covid data?
Is it the same as this?:
“43% of adults aged 16 and over had at least one longstanding medical condition
16% of children aged up to 15 years old had at least one longstanding medical condition”
or something more specific?
I’m not totally sure of the consistency of the definition, but we could start with this:
Any longstanding condition
| 16-24 | 25-34 | 35-44 | 45-54 | 55-64 | 65-74 | 75-84 | 85+ |
|---|---|---|---|---|---|---|---|
| % | % | % | % | % | % | % | % |
| 25 | 26 | 33 | 44 | 51 | 63 | 70 | 74 |
- [Health Survey for England, 2018: Longstanding conditions data tables]
3 Likes
Wow, quite sobering numbers there!
1 Like
Definitely worth a watch:

This seems to be by one Ivor Cummins. I can’t find much about him via Google (no Wikipedia entry) but it appears he is an Irish chemical engineer. Is he qualified to advise us on epidemiology and Covid-19 policy?
4 Likes
This is also certainly worth a read -
‘Current lockdown policies are producing devastating effects on short and long-term public health. The results (to name a few) include lower childhood vaccination rates, worsening cardiovascular disease outcomes, fewer cancer screenings and deteriorating mental health – leading to greater excess mortality in years to come, with the working class and younger members of society carrying the heaviest burden. Keeping students out of school is a grave injustice.’
2 Likes
Teenage girls (well they dud when my daughter was at school in the 80s) had a test to see if she had immunity to rubella, brcause of pregnancy. I’m not aware she has had rubella (it is a very mild disease, my mum told me) but she did have immunity.
2 Likes

This article suggests:
The UK government ‘Delay Phase’ states it will:
aim to minimise the social and economic impact, subject to keeping people safe
There is a subtle difference in wording but I doubt that accounts for the differences in suggested (policy). It’s really about whether ‘Focused Protection’ would work.
I think most western governments have concluded that herd immunity, even ‘Focused Protection’, cannot be achieved without an excessive amount of risk that the health service would ‘collapse’. There might be some element of career risk aversion (“nobody ever gets fired for doing the same thing as everyone else”) involved too.
2 Likes
I think you are right about the health system. Even without extra Covid loading, there is now a back log of treatment, operations and appointments for the NHS to deal with, as well as the threat of seasonal illnesseses looming. The ‘cracks’ are already evident:
The other problem with allowing those not at risk to live normally, while maintaining lockdown for the vulnerable, is that it feels very unjust in a society that trys to treat everyone equally.
2 Likes
We used to get blood tests at The Jenner health centre but now we have to go to a phlebotomy clinic. Just tried the 080 333 3217 number to book a test, my call is important to them but I was 59th in the queue! 
There’s a pretty interesting shakedown of this whole thing over at Wired.
3 Likes
Excellent article, thanks for sharing.
A while ago I tried to calculate the cost of lockdown to compare it to the current QALY cost of the forecasts of death numbers (what the NICE/NHS/ the state is willing prepared to pay for a citizens year of life) and couldn’t get close to what lockdown was going to cost. I put the decision making down to:
-
The precautionary principle - We knew very little about covid - worst case scenarios would be devastating.
-
Moral imperative - Morally, how could we do significantly less to protect our citizens than others in the developed world ?
-
Legacy risk - The idea of being the PM who oversaw 250K premature deaths is probably not what our current one had in mind.
3 Likes
Seems like a lot of the experts are fake too.
3 Likes